
The biologists who changed the face of assisted reproduction: the role of embryologists in developing reproductive medicine
The assisted reproduction in humans that we are familiar with today would not have been possible without the discoveries made over 70 years ago.
Biology-led progress
The first ever milestone in the history of assisted reproduction techniques was achieved in 1969 when biologist and 2010 Nobel Prize Winner for Medicine, Robert Edwards, managed to fertilise an ovum by bringing it into contact with spermatozoa in the laboratory.
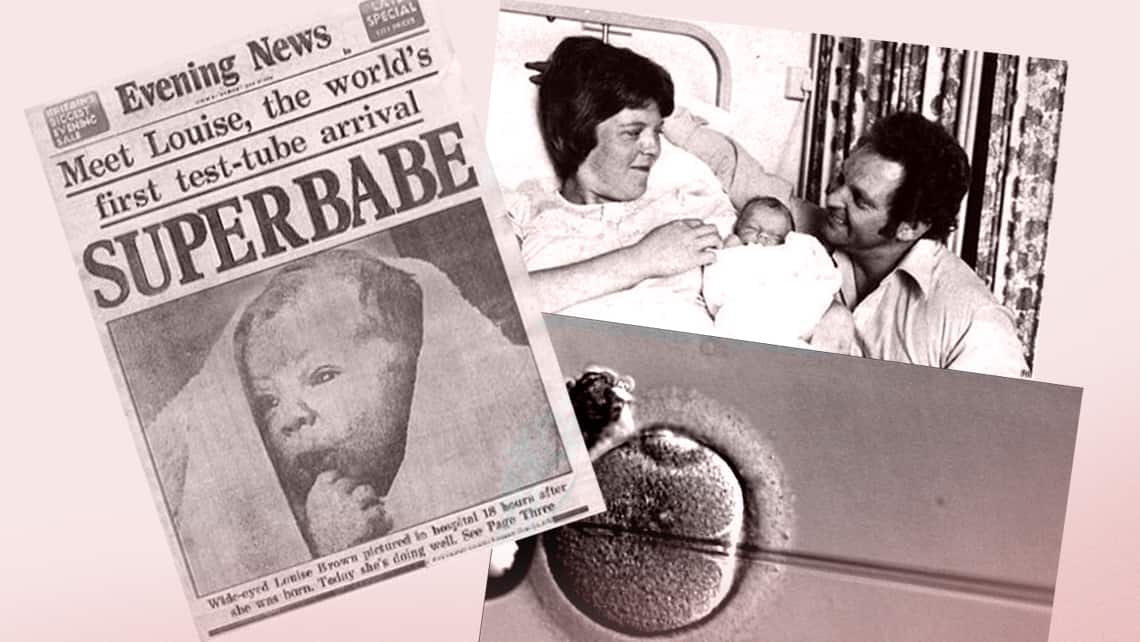
Following several attempts by the Patrick Steptoe and Robert Edwards team to successfully carry out transfer to the mother’s uterus, in 1978 they achieved the first ever birth thanks to this new technique known as in vitro fertilisation (IVF).
However, none of this would have been possible without the discovery of the main components of culture medium, which was made by Yves Menezo in 1976. The first IVF birth in Spain did not take place until 1984. It was performed by several specialists including biologist Anna Veiga. The first IVF birth at our clinic was recorded in 1988 and it was the first ever birth of its kind in the Valencian Community. Find out more about our clinic’s milestones.
Over time, in vitro fertilisation treatment was increasingly perfected and 1983 saw the first ever pregnancy following transfer of thawed embryos, which was achieved by the Trounson and Mohr team of biologists. However, this would not have been possible without the work that Wilmut and Whittingham had already done prior to that. These biologists published the first ever results of frozen and thawed mice embryos.
A few years later, in 1992, Gianpiero Palermo published news of the first ever successful pregnancy achieved using intracytoplasmic sperm injection into the ova (ICSI). The technique had been developed a few years earlier and it was a huge step forward in the treatment of male factor abnormalities because, in addition to facilitating fertilisation, only one spermatozoon per oocyte is required.
In addition, in 1990, pre-implantation genetic diagnosis of the embryo (DGP, PGT-A) was used to achieve the birth of offspring without X chromosome-related diseases. This milestone was achieved thanks to the work of the Handyside team, with essential input from biologist Kontogianni.
Assisted reproduction is a field of medicine that is constantly evolving and all the techniques have been perfected over the years. There is just one common objective: to improve the effectiveness of techniques and, in doing so, help form new families.
The functions of the embryo
When couples and women turn to an assisted reproduction clinic for help, achieving the dream of having a child is a question of impeccable coordination between all the members of an interdisciplinary team. The team includes embryologists who are experts that play a key role in successfully concluding assisted reproduction treatment.
Embryologists are most commonly qualified biologists. However, some are also veterinarians and pharmacists. They have acquired specialist knowledge of assisted human reproduction, genetics and scientific methodology, and are familiar with the legislation and bioethics associated with assisted reproduction. Since the field is continuously evolving, embryologists receive continuous training so that they can perform their job to the best possible standards.
Despite the fact that embryologists use all their knowledge to generate suitable embryos, it is a role that, on the whole, we are not particularly familiar with. Their work begins with a review of the patient’s clinical history so that they can gather a solid understanding of each case and apply the most suitable techniques. Once patients have embarked on the procedure journey, embryologists perform the following tasks in the laboratory:
- Sample analysis and processing of semen samples for use in the treatment;
- The search for the oocytes obtained in the follicular fluid and preparation in accordance with the applicable technique;
- Application of the most appropriate fertilisation technique for the patient (ICSI or IVF);
- Assessment of fertilisation and embryo development;
- Classification of embryos based on quality so that the very best embryo for transfer is selected;
- Participation during embryo transfer when the embryo is positioned inside the mother’s uterus;
- Embryo biopsies during blastocyst stage, if needed, depending on the type of treatment;
- Vitrification of viable oocytes or excess embryos that could be used in the future.
In addition to the above, embryologists are responsible for the upkeep and control of equipment and performing checks on environmental conditions (temperature, humidity, measuring volatile compounds) in order to ensure that there is an optimum system for embryo culture. Furthermore, when embryo transfer is performed, embryologists and doctors provide patients with precise information about embryo development. This is a key moment for giving patients the reassurance they need and answering any doubts that may have arisen during treatment.
In short, embryologists work on a daily basis with very sensitive material. Not only is it a huge professional undertaking; there is also an emotional component to their work.
Dr Antonio Urries, an embryologist and Chairman of ASEBIR, defines clinical embryologists as “the person looking after your baby, feeding it, watching over it day after day, minute after minute. He/she cares for all its needs so that it can grow strong and healthy, and does so with all the care and attention that he/she can. Just think, embryologists do this exactly nine months before a baby is born, at the very point in time when a child’s life is starting.”
Laura Martí, embryologist at Instituto Bernabeu.