
Ovarian cysts: What are they? Symptoms and treatment
One of the most common findings during a gynaecological check-up is the presence of ovarian cysts. This emergence of cysts is often unexpected and is generally a great cause for concern. Such concern is usually down to not knowing whether or not they are benign and whether or no they will require surgery.
Ovarian cysts are nothing more than liquid-filled lumps on the ovaries. This liquid may be fluid or dense and in most cases they are benign and functional cysts.
The term ‘functional’ refers to the fact that they are brought on by the hormonal changes that take place during the menstrual cycle itself and, therefore, tend to be more common during a woman’s childbearing years and less common during the menopause. Sometimes, a follicle which is due to rupture and release an egg during ovulation does not do so and so the liquid remains inside and continues to build up. Therefore, the cyst increases in size. These are what are known as follicular cysts and they generally disappear after a few months without the need for any type of treatment because they end up dissolving or bursting of their own accord.
Another possibility is that, following ovulation, the leftover sac (corpus luteum which usually disappears if the egg is not fertilised) instead increases in size and fills with liquid after gestation. This is known as a corpus luteum cyst and can reach quite a considerable size (>8 cm) but does tend to disappear of its own accord.
There are other non-functional cysts and amongst the most frequent are: endometrial cysts, which have a darker, chocolate-like content which is produced by the breakdown of the blood inside them; dermoid cysts, generated by secretions of a type of cell which is of embryo origin, can generate hair, teeth, cartilage and bone within the cyst and many others which are only diagnosed following a biopsy.
What are the symptoms?
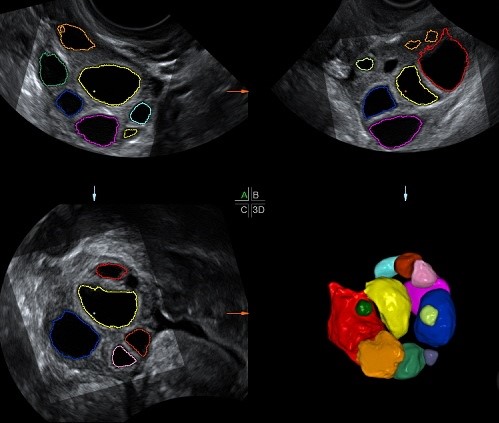
Most cysts do not have any symptoms and are generally unexpectedly detected during an ultrasound. However, those which are not detected this way generally cause slight discomfort when moving around or during sexual intercourse or alternatively cause slight, non-specific and continuous pelvic pain. On the other hand, a delayed period can be the only sign and the reason why the patient decides to visit the gynaecologist.
When should I become concerned? When a woman has an unexplained bloated abdomen or sudden, intense pelvic pain and nausea or sickness. This can be a sign of ovarian torsion in very large cysts or a rupture of a cyst with bleeding into the pelvis.
How can they be spotted?
If cysts are large, they can be detected during gynaecological check-ups. If they are not large, however, they can be seen quite clearly in abdominal or, preferably, vaginal ultrasounds.
Getting an understanding of the appearance of the cyst is important. The simple ones (only liquid) tend to be benign but in the complex or solid cysts (with a more dense content), the gynaecologist may need to determine if it is a benign or malignant tumour based on associated tests. For example, a computerised axial tomography scan (CAT scan), magnetic resonance imaging, tumour markers (such as the CA-125 or the ROMA index, amongst others), B-hCG (the pregnancy hormone) or laparoscopy. A biopsy of the cyst is the means of providing a definite diagnosis.
One of the tests that has recently become particularly relevant in terms of malignant diagnoses is the ROMA index (Risk Ovarian Malignancy Algorithm). It consists of a mathematical calculation which combines CA-125 serum levels and a new marker, HE4 (Human Epididymis Protein 4). This information, along with the patient’s age and menstrual status (pre or post menopause) means that patients may be classified as either High or Low Risk with reference to detecting ovarian cancer during surgery on the ovarian mass.
How should they be treated?
This will depend on the patient’s age, the symptoms and the size and characteristics of the cyst. Most simple, functional cysts disappear of their own accord and the gynaecologist will, therefore, prescribe ultrasound check-ups a few months later in order to confirm that this has indeed happened. If thing do not work out this way, contraception pills may be prescribed. Simple cysts are dealt with using surgery when they are large (>5-10 cm), persist and are accompanied by other symptoms, or when a complication arises (rupture leading to a haemorrhage or torsion).
The go-to surgical procedure is removal of the cyst whilst always taking care to carry out very careful procedures, particularly in women in childbearing age, and ensuring that as much of the healthy ovarian tissue as possible is preserved so that ovarian reserve is not jeopardised. Removal of ovaries should only occur during pre or post menopause phases in those cases in which the cyst is thought to be malignant or when, due to its considerable size, it is the only option. When the cyst is thought to be malignant, the most suitable treatment is a laparotomy (surgery with incision).
Prognoses for ovarian cysts tend to be favourable. However, it is very important to have regular gynaecological check-ups in order to quickly spot those cysts which do not follow benign behavioural patterns and do a close follow-up how they evolve.