
What is ovarian reserve? What role does it play in fertility?
Índice
- 1 What is ovarian reserve?
- 2 What role does it play in fertility?
- 3 How are ovarian reserve and ova quality linked?
- 4 How can I be told what my ovarian reserve is? What are normal values?
- 5 Does age have an impact on ovarian reserve?
- 6 What other factors can have an impact on ovarian reserve?
- 7 Poor ovarian reserve. What is it? What should I do?
What is ovarian reserve?
Ovarian reserve can be defined as the number of ova in a woman’s ovaries at any given point during her childbearing years.
In the case of men, spermatozoa production remains constant between puberty and senescence. Recent studies confirm that spermatozoa quantity and quality can diminish over time. However, men generally remain fertile throughout their lives. Women, on the other hand, are born with a limited number of ova and ova loss is an exponential and irreversible process that begins when a woman is born and continues right up until the menopause.
Therefore, in terms of reproduction, age has little impact in men but is a vital factor in women.
What role does it play in fertility?
Poor ovarian reserve is not strictly a cause of sterility. Young women with poor ovarian reserve can get pregnant naturally. However, it is directly linked to the number of oocytes that are recovered following ovarian stimulation and to the amount of medication that has to be prescribed. As such, the number of ova that are recovered from a patient with poor ovarian reserve is slightly lower than those recovered from a woman with a normal or high ovarian reserve. This is true even when the patient is prescribed elevated doses of gonadotropins.
Since the number of ova that are recovered is directly linked to the number of embryos that can be transferred to the uterus, the more ova that are available, the greater the chances of obtaining one or more good quality embryos. This, in turn, increases the chances of pregnancy.
The two main factors that have an impact on the success of assisted reproduction treatment are ovarian reserve and the female patient’s age. Therefore, understanding the condition of a patient’s ovarian reserve is absolutely essential to providing her with a prognosis and appropriate advice.
[yframe url='https://www.youtube.com/watch?v=HKxT0qK-Y4Y&t'] How are ovarian reserve and ova quality linked?
Ovarian reserve is an ova quantity marker, not an indication of quality. Age is the leading marker for ovarian quality. Whilst age-related diminished ovarian reserve is more common in patients who are 40 years of age or older, the quality of ova in young patients with poor ovarian reserve tends to be correct for their age. Therefore, diminished ovarian reserve is not always an indication of poor-quality ova.
How can I be told what my ovarian reserve is? What are normal values?
There are a number of available diagnostic tests for assessing ovarian reserve. The ones that are most commonly used in clinical practice include measuring anti-Müllerian hormone levels and performing antral follicle counts.
Antral follicle counts
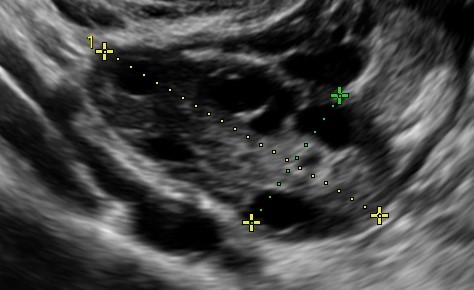
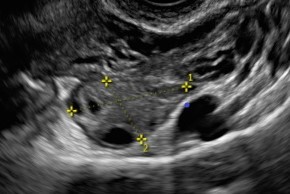
The best option is a vaginal ultrasound scan performed between days 2 and 5 of the menstrual cycle. However, it can also be performed on any day of the cycle. The follicles in both ovaries between 2 and 10mm in length are counted.
- Normal ovarian reserve: between 10 and 20 follicles are observed.
- Poor ovarian reserve: fewer than 10 follicles in both ovaries are observed.
- Elevated ovarian reserve: over 20 follicles are observed.
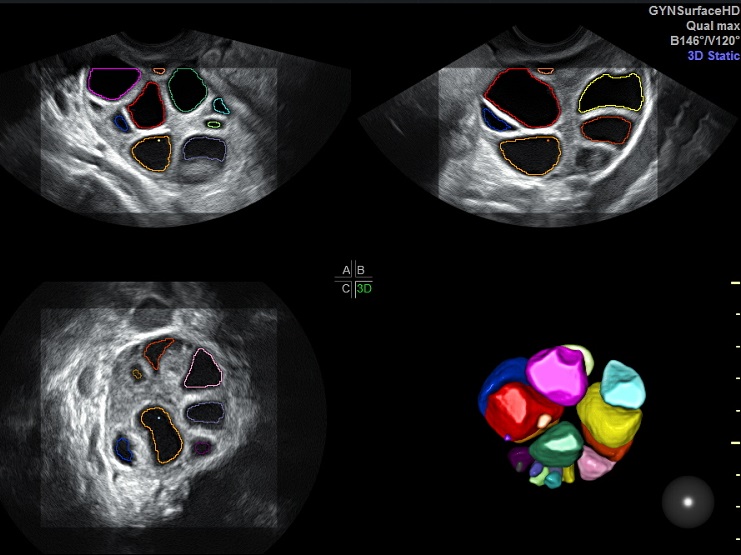
Nowadays, the count can also be performed using SonoAVC three-dimensional ultrasound scan technology.
Anti-Müllerian hormone (AMH) analyses
Hormone levels are assessed using a blood sample taken on any day of the menstrual cycle. Preferably, this needs to be performed when the patient is not taking oral contraception. The measurement can be taken in nanograms/millilitre (ng/ml) or picomoles/litre (pmol/L)
- Normal ovarian reserve: AMH levels between 1 and 3 ng/ml or 7-21 pmol/L
- Poor ovarian reserve: AMH levels under 1 ng/ml or 7 pmol/L
- Elevated ovarian reserve: AMH levels in excess of 3 ng/ml or 21 pmol/L
FSH and oestradiol serum analyses
This must be performed between days 2 and 5 of the cycle. An FSH level in excess of 10 Iu/ml and/or an oestradiol level in excess of 60 pg/ml is an indication of poor ovarian reserve.
Dynamic tests for assessing ovarian reserve
These tests include, for example, the clomiphene citrate test, the gonadotropins test or the GnRH analogues test (currently not performed in standard clinical practice).
Does age have an impact on ovarian reserve?
Ovarian reserve depends entirely on a woman’s age. Women only generate ova between week 12 and month 5 of pregnancy. They are also born with a limited number of ova for their entire life. Only around 400 of these ova are ovulated from puberty onwards. That is, one for each menstrual cycle. The remainder suffer from atresia and do not ovulate. Women are most fertile between approximately 18 and 30 years of age. This is when the best quality oocytes ovulate. Only a few dozen oocytes remain when a woman reaches the menopause.
What other factors can have an impact on ovarian reserve?
In addition to age, there are a number of factors that can decrease ovarian reserve levels prematurely. These include:
- Treatment for cancer, including radiotherapy and chemotherapy.
- Genetic disorders such as abnormalities in the karyotype or FMR1 premutation or fragile X syndrome carriers.
- Cases of premature menopause amongst family members.
- Surgery performed on the ovaries.
- Gynaecological diseases such as endometriosis.
- Autoimmune diseases.
- Smoking.
- Exposure to contaminants or endocrine disruptors.
Poor ovarian reserve. What is it? What should I do?
A patient is understood to have poor ovarian reserve if she has an abnormal antral follicle count and/or poor AMH levels. If, in addition, the patient is over 40 years old, her reproductive prognosis worsens even more. This is the case even when using assisted reproduction techniques such as in vitro fertilisation (IVF).
It is important to highlight that there are absolutely no symptoms associated with poor ovarian reserve in the majority of cases. However, one of the most common symptoms is shorter menstrual cycles.
So, several essential aspects for reproduction health should be taken into account:
- Refraining from delaying pregnancy. Even when a patient has a normal or elevated ovarian reserve, her chances of becoming a mother drastically decrease after 35 years of age.
- Should a woman choose to delay getting pregnant for whatever reason (financial or social factors and so on), or if there are a range of risk factors, she can choose to have ovarian stimulation treatment and perform oocyte vitrification in order to retain the quality of her ova and ‘put her biological clock on hold’. This treatment is by no means a guarantee of getting pregnant in the future. However, it can help increase a woman’s chances, particularly if she chooses to delay having children until after 35 to 37 years of age.
- If a woman suspects that she may have poor ovarian reserve, she should put herself in the hands of a specialist unit in order to get appropriate advice on reproduction.
At Instituto Bernabeu, we design specific and personalised poor ovarian reserve protocols for patients in order to optimise their response to ovarian stimulation. We are acutely aware that a patient’s chances of success decrease as time goes by. Likewise, we have several lines of research in order to improve patients’ reproduction prognosis as quickly as possible.
Dr Cristina García-Ajofrín, a gynaecologist atInstituto Bernabeu.